III. How Epic TEFCA Works (Architecture Explained)
A. Data exchange flow
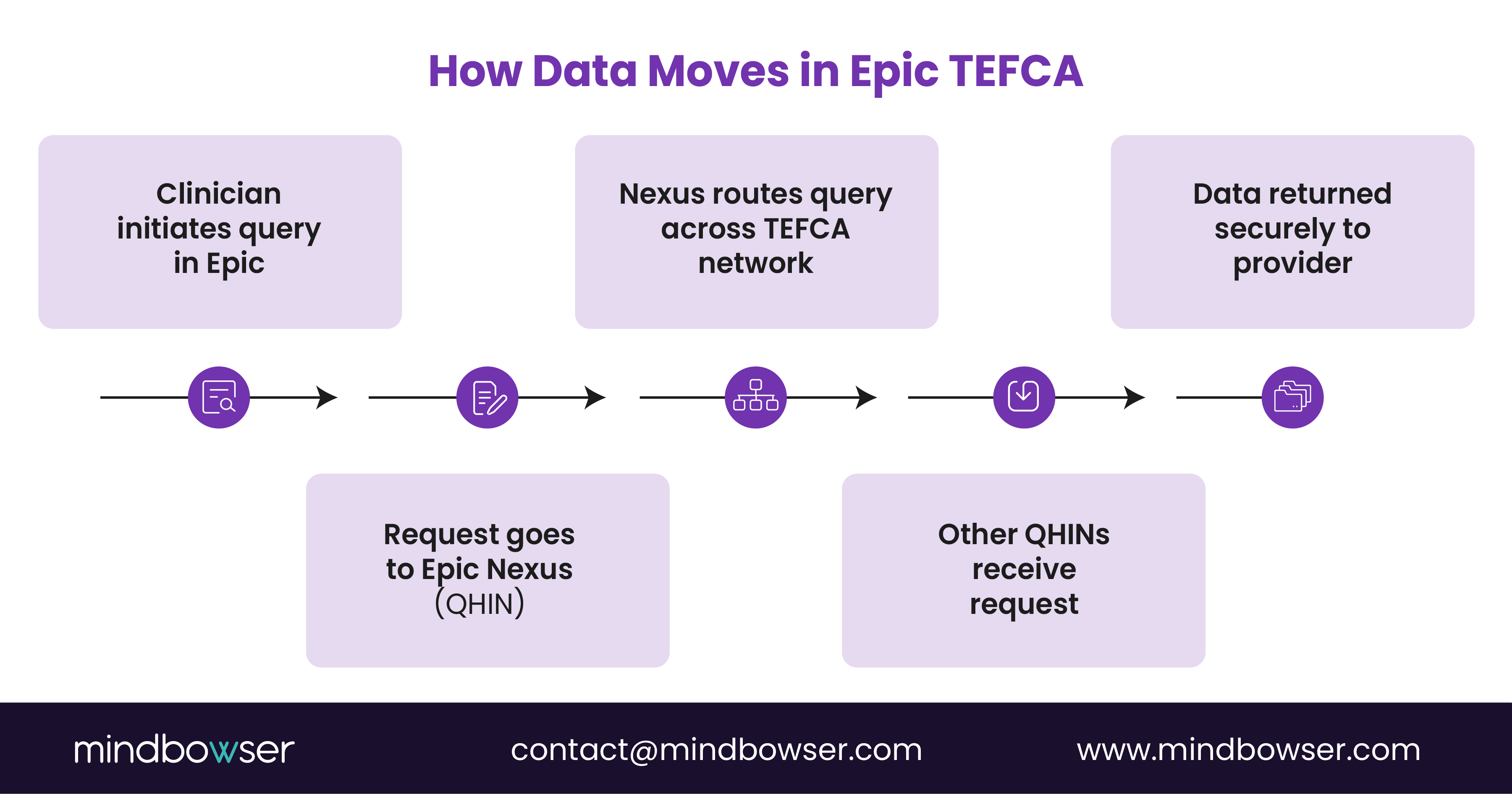
How does data actually move in an Epic TEFCA environment? Let’s break it down from a real operational lens.
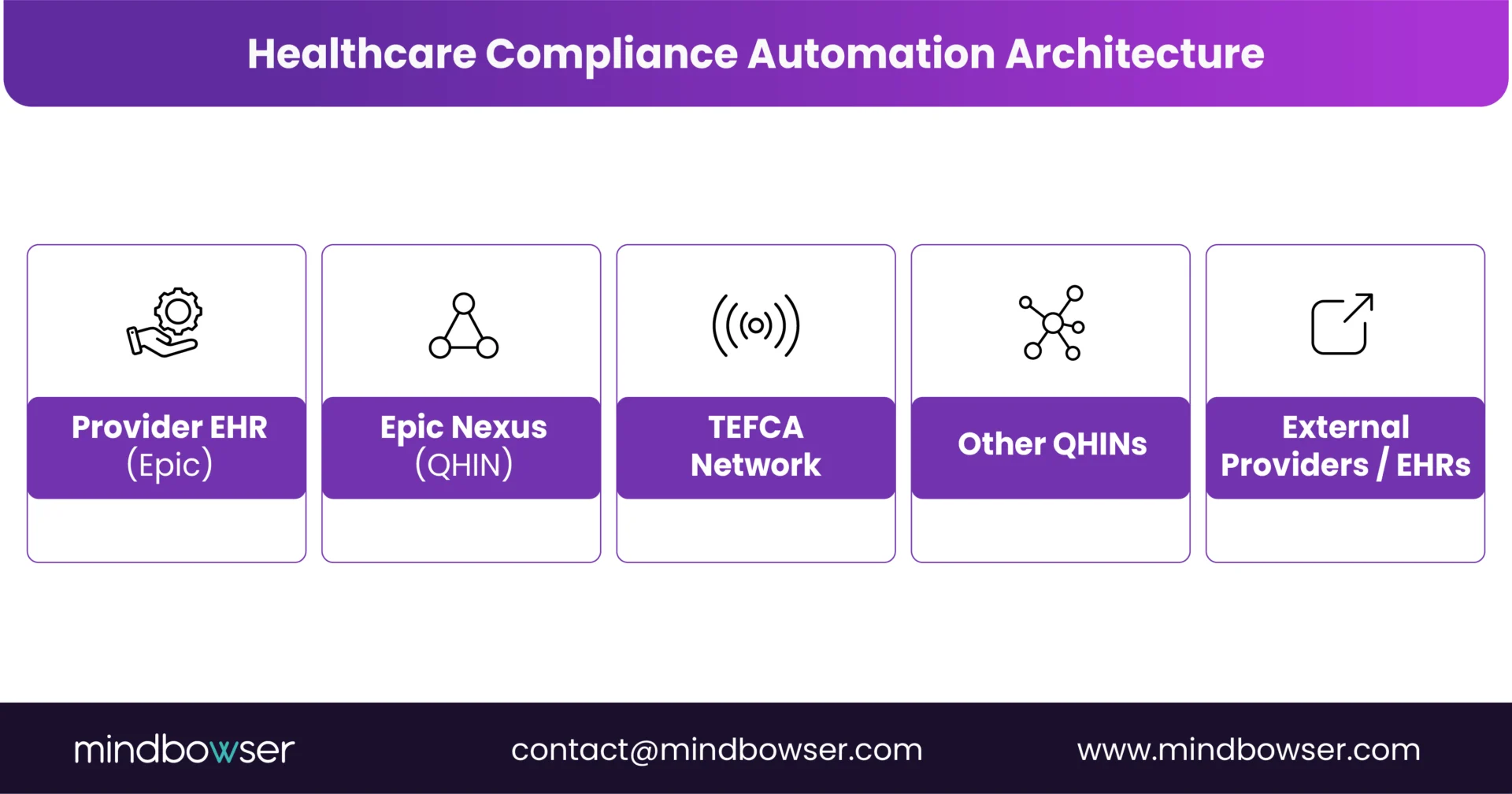
A clinician initiates a query inside an Epic EHR. That request doesn’t go directly to another hospital. Instead, it follows a structured path:
- The provider uses Epic EHR to initiate a patient query
- The organization connects to Epic Nexus (QHIN)
- Epic Nexus routes the request across the TEFCA network
- Other QHINs receive and process the query
- Data is returned securely to the requesting provider
This is not a point-to-point exchange. It is brokered interoperability. Think of QHINs as air traffic control. They don’t own the planes. They coordinate the movement.
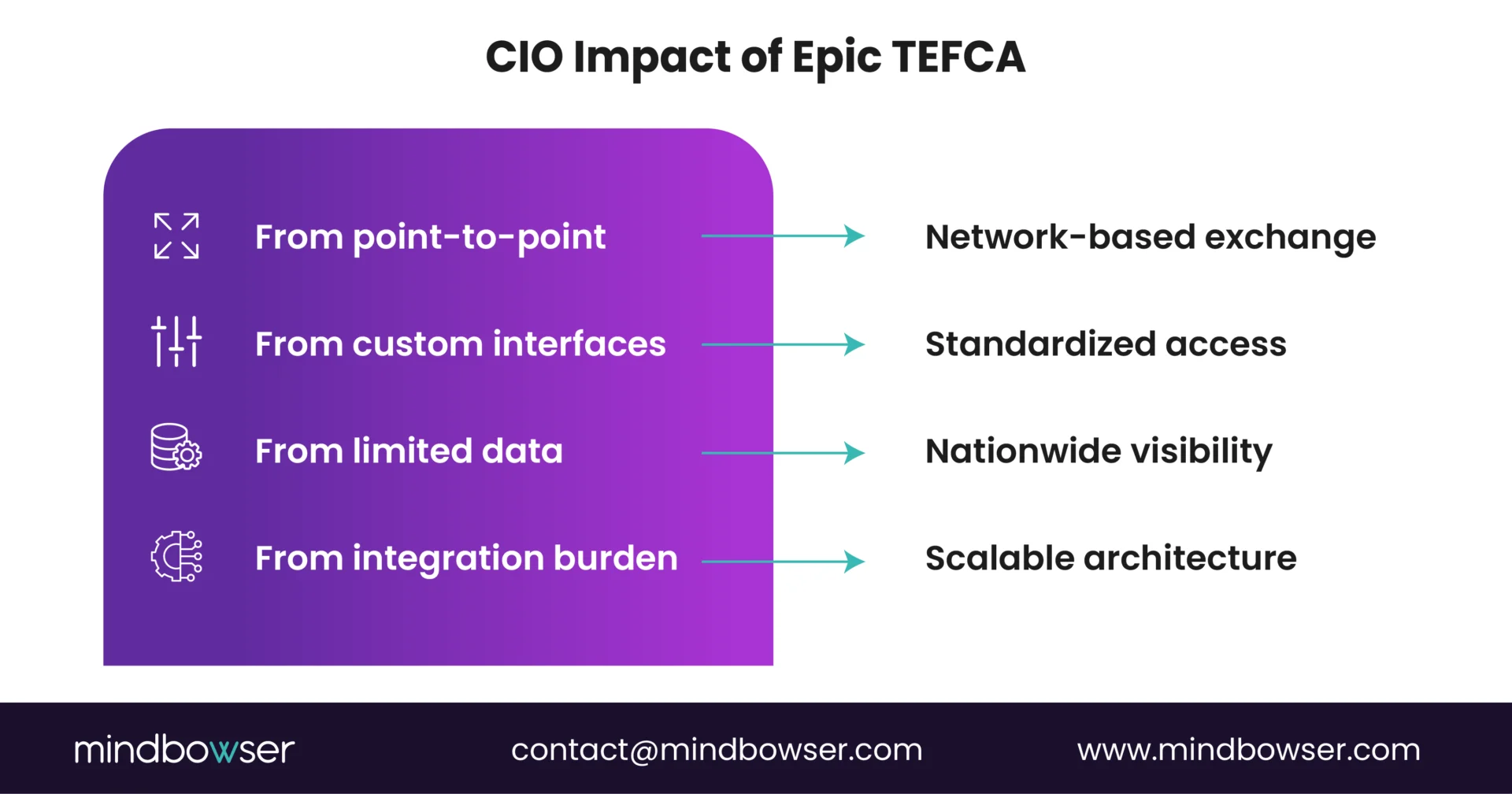
TEFCA standardizes not just connectivity, but how queries are routed, responded to, and governed. For CIOs, this matters because it shifts architecture from interface-heavy designs to network-based orchestration. Fewer interfaces. More intelligence in the network layer.
B. Exchange use cases supported today
TEFCA is not a future state. It already supports concrete, high-value use cases.
1. Treatment queries — Clinicians can request patient records from external organizations to support care decisions. This reduces blind spots. It also reduces duplication. According to industry estimates, nearly 20% of healthcare spending is tied to unnecessary or duplicate services, much of it driven by a lack of accessible data. TEFCA directly addresses this gap.
2. Patient access to records — Patients can retrieve their own health data through TEFCA-enabled applications. This is enabled through Individual Access Services (IAS). Patients are no longer dependent on a single provider portal. They can access longitudinal records across systems.
3. Public health reporting — TEFCA supports standardized data exchange with public health agencies. This improves reporting consistency, timeliness of data submission, and population health visibility.
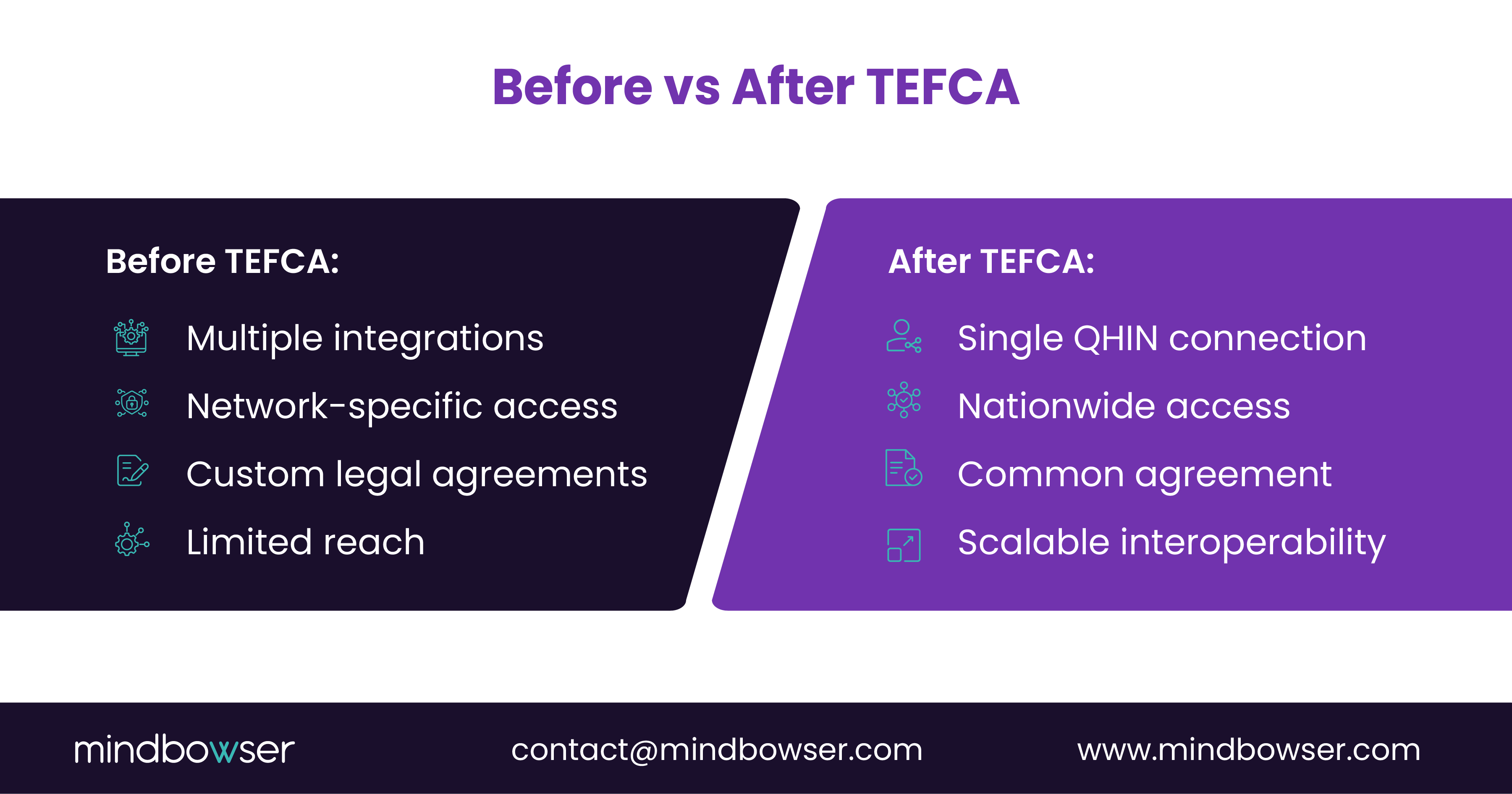
Here’s the shift. Before TEFCA: use-case-specific integrations. With TEFCA: a shared infrastructure supporting multiple use cases.
C. Architecture implications
This is where executives need to lean in. Epic TEFCA is not just a connectivity upgrade. It is an architecture decision point.
Ask yourself:
- Is your integration layer built for network-based exchange or interface-based exchange?
- Are your APIs aligned with FHIR-first patterns?
- Can your systems handle query-based retrieval vs batch-based data movement?
Because TEFCA favors:
- Real-time queries over file transfers
- Standardized APIs over custom interfaces
- Governance-driven exchange over ad-hoc sharing
Short sentence. Big implication. Epic TEFCA replaces fragmented data exchange paths with a structured, QHIN-driven architecture. Organizations that adapt their integration model will move faster, reduce duplication, and unlock real-time access to nationwide patient data.
IV. Why Epic’s TEFCA Adoption Is a Turning Point for Healthcare
A. Key impacts
What changes when interoperability finally reaches national scale? Not marginal gains. Structural shifts.
Epic’s adoption of TEFCA through Nexus is not just another integration milestone. It marks the point where interoperability begins to behave like infrastructure rather than a feature. Here is what that unlocks.
- Nationwide data liquidity — Patient data is no longer confined to regional networks or vendor ecosystems. It flows across QHINs, making longitudinal records accessible regardless of geography. For CMIOs, this means better-informed clinical decisions. For CIOs, it means fewer gaps in data availability.
- Reduced duplicate testing — When clinicians can access prior labs, imaging, and encounters, unnecessary repeat procedures drop. Nearly 20% of U.S. healthcare spending is attributed to waste, including redundant services. TEFCA directly targets that inefficiency.
- Faster care coordination — Transitions of care improve when receiving providers have immediate access to patient history. Discharge today. Follow up tomorrow. No data lag. That continuity matters in value-based care models.
- Unified patient access — With TEFCA’s Individual Access Services (IAS), patients gain broader control over their health data across systems. Not five portals. One longitudinal view.
B.Why This Matters
TEFCA extends integrated interoperability across healthcare providers. Simple statement. Big consequence.
Because when interoperability becomes consistent:
- Care teams collaborate faster
- Data fragmentation decreases
- Patient experiences improve
Here is the contrast worth noting. Before TEFCA, interoperability was selective and network-bound. With Epic TEFCA, interoperability becomes expected and nationwide.
There is also a market signal embedded here. When Epic, with its vast provider footprint, operationalizes TEFCA:
- Other vendors must align
- Health systems must adapt
- Digital health companies must integrate differently
No one operates in isolation anymore. Epic’s TEFCA adoption marks the shift from fragmented interoperability to nationwide data liquidity. Organizations that align early will reduce waste, improve care coordination, and position themselves for the next wave of connected healthcare.
V. Epic TEFCA vs Previous Interoperability Networks (Carequality, CommonWell)
A. Why the industry is transitioning
If interoperability already existed, why did the industry need TEFCA? Because existing networks solved connectivity. Not consistency.
For years, healthcare relied on frameworks like Carequality and CommonWell to exchange data. They played a critical role in advancing interoperability. But they evolved independently, with different governance models, technical approaches, and participation rules. The result? Progress. But also fragmentation.
Here’s how the shift is unfolding at an executive level:
- Governance — Carequality and CommonWell operate as private frameworks with their own rules and agreements. TEFCA introduces federal governance, creating a single, standardized model across all participants. One rulebook. Nationwide alignment.
- Scope — Legacy networks often depend on who is connected to whom. TEFCA expands this into a network-of-networks, where QHINs interconnect and extend reach beyond individual frameworks. Reach is no longer limited by network boundaries.
- Patient data access — While previous networks supported data exchange, TEFCA formalizes Individual Access Services (IAS), enabling patients to retrieve their health data across systems through approved applications. This shifts control closer to the patient.
| Capability | Carequality / CommonWell | TEFCA |
|---|---|---|
| Governance | Private, network-specific | Federal, standardized |
| Connectivity | Network-to-network agreements | QHIN-based nationwide exchange |
| Scalability | Dependent on participation | Designed for a national scale |
| Patient Access | Limited standardization | Built-in IAS framework |
B. Context
Epic historically relied heavily on Carequality to enable cross-network exchange. It worked well within defined ecosystems and enabled broad data sharing among participating organizations. But as interoperability demands expanded, limitations became clearer:
- Multiple frameworks to manage
- Inconsistent policies across networks
- Gaps in nationwide coverage
TEFCA addresses these gaps by introducing a unifying layer above existing networks. It does not replace them overnight. It standardizes how they connect. TEFCA is less about replacing networks and more about connecting them under a single framework. That nuance matters.
For CIOs, this is not a rip-and-replace decision. It is an evolution of the interoperability strategy.
Here is the strategic inflection point. Before TEFCA: choose networks and manage integrations. With TEFCA, connect to a QHIN and access all participating networks. Fewer decisions. Broader reach.
TEFCA represents the maturation of interoperability from fragmented, network-specific exchange to a unified national framework. Organizations that continue to rely only on legacy networks risk slower scaling and limited reach in a QHIN-driven future.
VI. What TEFCA Means for Health Systems Using Epic
A. Benefits of Epic TEFCA
You’re a CIO at a 300-bed health system. A patient just transferred from another state. What do you expect to see in your EHR? Today, many would say: partial records. Delays. Gaps.
With Epic TEFCA, that expectation changes.
Nationwide patient record access — Through Epic Nexus, your clinicians can retrieve patient data from across QHIN-connected networks. Not just regional. National. That means:
- Prior admissions from out-of-state systems
- Medication histories from unaffiliated providers
- Diagnostic results from external labs
Care decisions become more complete. Faster too.
- Reduced integration complexity — Think about your current integration backlog. Dozens of interfaces. Each has its own mapping, testing cycle, and maintenance overhead. Now imagine telling your team: We connect once. The network handles the rest. That is the TEFCA model. Fewer interfaces to build. Fewer to maintain. Less operational drag.
- Improved public health reporting — Public health reporting often feels reactive. Data requests come in. Teams scramble. Formats vary. TEFCA introduces a more standardized pathway, making it easier to share data with public health agencies, respond to reporting requirements, and support population health initiatives.
- Stronger compliance alignment — TEFCA is federally aligned. That matters. Instead of interpreting multiple frameworks, your organization aligns with a single national model for data exchange, privacy, and governance. Less ambiguity. Clearer direction.
B. Strategic implications for CIOs
Now step into a different scenario. You are planning your interoperability roadmap for the next 24 months. Two paths emerge.
Path 1: Continue investing in point-to-point integrations. Expand existing network connections. Maintain the status quo.
Path 2: Align with TEFCA. Connect through Epic Nexus. Shift toward QHIN-based exchange.
Which one scales better? This is the decision TEFCA forces.
New interoperability pathways — Instead of asking, “Which network should we join?” the question becomes: “How do we maximize value from our QHIN connection?” That is a different mindset.
Simplified vendor integrations — Vendors that are TEFCA-ready can integrate faster. You are no longer evaluating each vendor’s custom integration capability. You are assessing their ability to operate within a QHIN ecosystem. That shortens procurement cycles.
Expanded data-sharing use cases — Once connected, new use cases emerge:
- Cross-network care coordination
- Longitudinal patient records for value-based care
- Broader analytics across diverse patient populations
Here’s the subtle shift. Interoperability moves from project-based execution to platform-based capability.
Now the uncomfortable question. If a competing health system adopts TEFCA early and you delay, what happens? They access more data. They coordinate care faster. They reduce duplication sooner. You operate with less visibility. That gap compounds.
TEFCA is not forcing change overnight. But it is setting direction. And direction, over time, becomes default.
VII. What Digital Health Companies Must Know About Epic TEFCA Integration?
A. Key integration considerations
You’re a Series B digital health founder. Your product needs data from 50+ health systems. How many integrations are you planning? If your answer is “50,” you are already behind.
TEFCA changes the integration equation. Instead of building one-off connections to each provider or EHR, digital health platforms can connect via a QHIN to access a broader network. But that does not mean plug-and-play. The architecture still matters.
Here is what teams must get right.
- QHIN onboarding — You do not connect to TEFCA directly. You are onboarded via a QHIN such as Epic Nexus or another designated network. This involves technical validation, security compliance checks, and legal alignment under the Common Agreement. It is structured. And it is non-negotiable.
- FHIR APIs as the foundation — TEFCA increasingly aligns with FHIR-based exchange patterns, especially for patient access and modern app integrations. If your platform is not FHIR-native, integration becomes slower and more brittle. Simple question: Are your APIs ready for query-based retrieval at scale?
- Data governance and consent management — Access is not unrestricted. Digital health platforms must handle patient consent workflows, data use restrictions, and audit and traceability requirements. Miss this, and integration stalls at the compliance layer.
- Security requirements — TEFCA enforces strict expectations around identity verification, data encryption, and access controls. This is not just about passing a security review. It is about maintaining trust across a national network.
B. Developer perspective
Now step into your engineering team’s shoes. They are used to building custom integrations: HL7 feeds for one system, FHIR APIs for another, custom mappings for a third. It works. But it does not scale cleanly.
TEFCA introduces a different model. Connect once. Expand everywhere.
When you integrate with one QHIN:
- You gain access to all participants connected through that QHIN
- You reduce the need for repeated EHR-specific integrations
- You standardize how queries and responses are handled
That is a massive shift in developer effort.
But here is the nuance. TEFCA simplifies connectivity, not product design. You still need to normalize incoming data, handle variations in clinical workflows, and design user experiences that make sense of aggregated data. Technology solves access. Product still solves value.
You are building a remote patient monitoring platform. You want to pull vitals, labs, and encounter data from multiple providers. Without TEFCA: Multiple EHR integrations, long onboarding cycles, high maintenance overhead. With TEFCA: Single QHIN integration, broader data access, and faster expansion into new markets.
Which model gets you to scale faster? TEFCA does not remove complexity. It relocates it. From connection building to data orchestration and experience design. That is where the winners will differentiate.
VIII. Challenges and Open Questions Around Epic TEFCA
A. Key challenges
If TEFCA simplifies interoperability, why isn’t everyone fully aligned already? Because simplification at the network level often exposes complexity at the operational level.
- Implementation complexity — Connecting to a QHIN is not just a switch you flip. It requires internal architecture alignment, workflow adjustments for clinicians, and testing query-response behaviors across systems. The network is standardized. Your internal systems may not be. That gap shows up quickly.
- Data governance challenges — Now imagine a different situation. A patient’s data is available across multiple networks. Different organizations have contributed to that record. Who governs access? Who ensures appropriate use? TEFCA defines rules, but execution happens at the organizational level. This introduces questions around data ownership vs data stewardship, consent enforcement across networks, and audit readiness. Governance is no longer local. It is distributed.
- Vendor ecosystem alignment — Here is another friction point. Not every vendor is equally TEFCA-ready. Some platforms support FHIR well, align with QHIN-based exchange, and adapt quickly. Others lag. Now you are managing a mixed ecosystem. Part TEFCA-enabled. Part legacy. That creates architectural tension. Do you wait for vendors to catch up? Or build interim layers to bridge the gap?
- Policy and evolution uncertainty — TEFCA is still evolving. Use cases will expand. Rules may adapt. Participation will grow. For executives, this raises a strategic question: How do you design for a framework that is still maturing? Build too rigidly, and you risk rework. Stay too flexible, and you risk delays. Finding that balance is not trivial.
A competing health system embraces TEFCA aggressively. They invest early, adapt workflows, and align vendors. You take a wait-and-watch approach. Six months later: They access broader patient data. Their care coordination improves. Their integration backlog shrinks. You are still evaluating. That gap is not just technical. It becomes competitive.
Interoperability is no longer about whether systems can connect. It is about how well organizations operationalize that connection. TEFCA introduces a new layer of capability. But capability without execution does not create value. That is where leadership decisions matter most.
IX. How Mindbowser Builds Custom EHRs with Epic Integration Capabilities
What happens when your platform must integrate with Epic, multiple HIEs, and TEFCA at the same time? This is not hypothetical.
A digital health company wants to launch across three states. Each region has different provider networks. Some use Epic. Others rely on regional HIEs. Now TEFCA enters the mix. Your team faces a choice: Build fragmented integrations. Or design for convergence from day one. This is where architecture matters.
A. Our approach
We design systems assuming Epic TEFCA is the center of gravity, not an edge case.
1. Epic-first interoperability architecture
We start where most patient data lives. SMART on FHIR applications embedded within Epic workflows, Epic App Orchard integrations for secure, governed access, HL7 and FHIR pipelines to handle both legacy and modern exchange. This ensures your solution works inside the clinician’s reality, not outside it.
2. TEFCA-ready data exchange
Instead of retrofitting later, we build for QHIN compatibility upfront. That includes query-based data retrieval models aligned with TEFCA, interoperability layers that can connect to QHINs like Epic Nexus, and governance-aware data handling for compliance readiness. So when TEFCA expands, your platform does not need to catch up. It is already aligned.
3. Digital health platform integrations
Now consider a care coordination platform operating across multiple hospitals. We enable Remote Patient Monitoring (RPM) integrations, care coordination systems spanning provider networks, and patient engagement apps that pull longitudinal data. The goal is simple. One platform. Multiple ecosystems. No fragmentation.
4. AI-powered clinical workflows
Data access is only step one. Action is where value is created. We layer intelligence into workflows: AI Medical Summary for faster clinical context, CarePlan AI to support coordinated treatment decisions, AI Readmission Risk to flag high-risk patients early, RPMCheck AI for proactive remote monitoring.
Now imagine a clinician opening Epic and seeing not just data, but prioritized insights across networks. That is where interoperability starts driving outcomes.
In a TEFCA-driven world, custom EHRs and platforms that align early will move faster, integrate cleaner, and scale wider. Others will spend cycles catching up.
PakarPBN
A Private Blog Network (PBN) is a collection of websites that are controlled by a single individual or organization and used primarily to build backlinks to a “money site” in order to influence its ranking in search engines such as Google. The core idea behind a PBN is based on the importance of backlinks in Google’s ranking algorithm. Since Google views backlinks as signals of authority and trust, some website owners attempt to artificially create these signals through a controlled network of sites.
In a typical PBN setup, the owner acquires expired or aged domains that already have existing authority, backlinks, and history. These domains are rebuilt with new content and hosted separately, often using different IP addresses, hosting providers, themes, and ownership details to make them appear unrelated. Within the content published on these sites, links are strategically placed that point to the main website the owner wants to rank higher. By doing this, the owner attempts to pass link equity (also known as “link juice”) from the PBN sites to the target website.
The purpose of a PBN is to give the impression that the target website is naturally earning links from multiple independent sources. If done effectively, this can temporarily improve keyword rankings, increase organic visibility, and drive more traffic from search results.
Comments are closed, but trackbacks and pingbacks are open.