A rural hospital deploying Remote Patient Monitoring in 2026 faces the same seven-layer technology stack a 500-bed health system uses, plus three constraints that completely change the architectural choices. A meaningful share of patients lack modern-benchmark broadband , the FCC’s 2024 Section 706 Report documents roughly 16.9 percent of rural Americans without 25/3 Mbps access and approximately 28 percent without 100/20 Mbps. The IT team is one or two people. Medicare cost-based reimbursement covers operating cost but does not fund the initial capital.
Those three constraints have blocked rural RPM scale for a decade. The technology existed. The reimbursement existed. The clinical evidence existed. What did not exist was a capital path, a cellular-first architecture maturity, and an operational model that fit rural facility staffing. All three conditions changed between 2023 and 2026. Cellular-enabled medical-grade devices matured. Device-agnostic ingestion platforms emerged. And in December 2025, the Rural Health Transformation Program awarded $50 billion across all 50 states with RPM expansion as an explicit funded activity in multiple state plans.
The RPM spending trajectory underscores why rural programs cannot wait. The Peterson Health Technology Institute’s April 2025 report “Evolving Remote Monitoring: An Evidence-Based Approach to Coverage and Payment” documents that Medicare RPM spending grew from $6.8 million in 2019 to $194.5 million in 2023 , a 28x increase in four years. PHTI’s analysis found, critically, that RPM services were most heavily used by non-white urban dually-eligible populations rather than by rural populations the technology was supposed to serve. RHTP funding is explicitly structured to close that rural-uptake gap; the rural hospitals that launch in the Q3 2026 – Q1 2027 procurement window are positioning against both the technology opportunity and the policy signal that rural populations should see this growth next.
The question shifted. It is no longer “can we afford rural RPM.” It is “can we execute the 90-day launch without the common failure modes that kill rural RPM programs in months two and three.”
This guide covers the architecture rural RPM actually requires, why cellular-first is non-negotiable, which clinical use cases produce measurable revenue, the Medicare RPM billing mechanics that make the program financially sustainable, the 90-day launch sequence, and the RHTP funding pathway that closes the capital gap.
For the broader seven-component CAH technology stack, see Technology Stack for a 25-Bed Rural Hospital. For RPM as part of the Hospital-at-Home platform, see Hospital at Home: The Complete Technology Platform Guide.
What Does Rural RPM Architecture Actually Require?
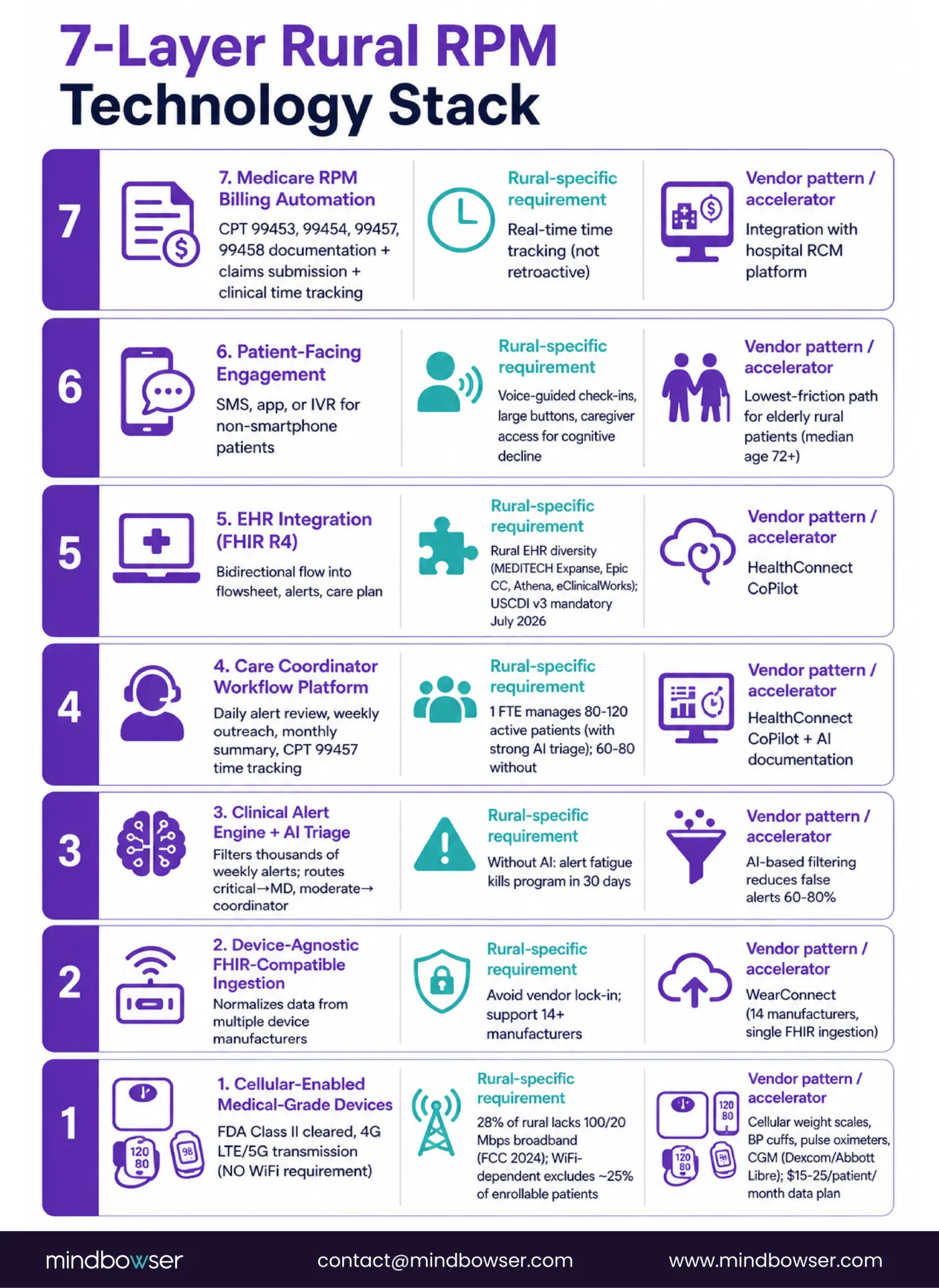
Rural RPM has seven technology layers. Each has a vendor market. Each has rural-specific requirements that differ from urban deployment patterns.
- Layer 1: Cellular-enabled medical-grade devices. FDA Class II cleared devices that transmit data over cellular networks without requiring home WiFi. Device categories vary by clinical use case (pulse oximeters, blood pressure cuffs, weight scales, continuous glucose monitors, peak flow meters, ECG patches).
- Layer 2: Device-agnostic FHIR-compatible ingestion layer. The abstraction layer that normalizes data from multiple device manufacturers into a single data stream compatible with EHR integration. This is where architectural discipline separates sustainable platforms from vendor-lock-in traps. Our WearConnect accelerator handles 14 device manufacturers through a single FHIR-compatible ingestion layer.
- Layer 3: Clinical alert engine with AI-based triage filtering. Without AI filtering, a rural RPM program managing 100 patients produces thousands of alerts per week, most clinically irrelevant. Alert fatigue becomes the operational bottleneck within 30 days. AI filtering reduces false alerts by 60-80 percent and routes clinically significant alerts to the care coordinator.
- Layer 4: Care coordinator workflow platform. The interface where a care coordinator manages 80-120 active RPM patients. Daily alert review, weekly patient outreach, monthly clinical summary generation for physician review, and Medicare RPM time tracking for CPT 99457 billing.
- Layer 5: EHR integration. Rural hospitals run MEDITECH Expanse, Epic Community Connect, Athena, or eClinicalWorks. RPM data must flow into the patient’s EHR flowsheet, alert history, and care plan. Manual data entry between RPM platform and EHR kills the business case. FHIR R4 integration is the standard, with USCDI v3 mandatory July 2026 for certified health IT.
- Layer 6: Patient-facing engagement interface. SMS, app, or IVR for non-smartphone patients. Elderly rural patients need the lowest-friction engagement path. Voice-guided check-ins, large-button interfaces, caregiver access for patients with cognitive decline.
- Layer 7: Medicare RPM billing automation. CPT 99453, 99454, 99457, 99458 documentation and claims submission. Time tracking for clinical staff interactions. Integration with the hospital revenue cycle management platform.
Rural RPM programs that skip or shortcut any layer fail predictably. The programs that execute all seven, with rural-specific architecture choices at each layer, scale.
Why Cellular-First Architecture Is Non-Negotiable for Rural RPM
The rural broadband gap is not a statistical footnote. It is the architectural constraint that determines whether a rural RPM program enrolls its target patient population or excludes a meaningful share of it.
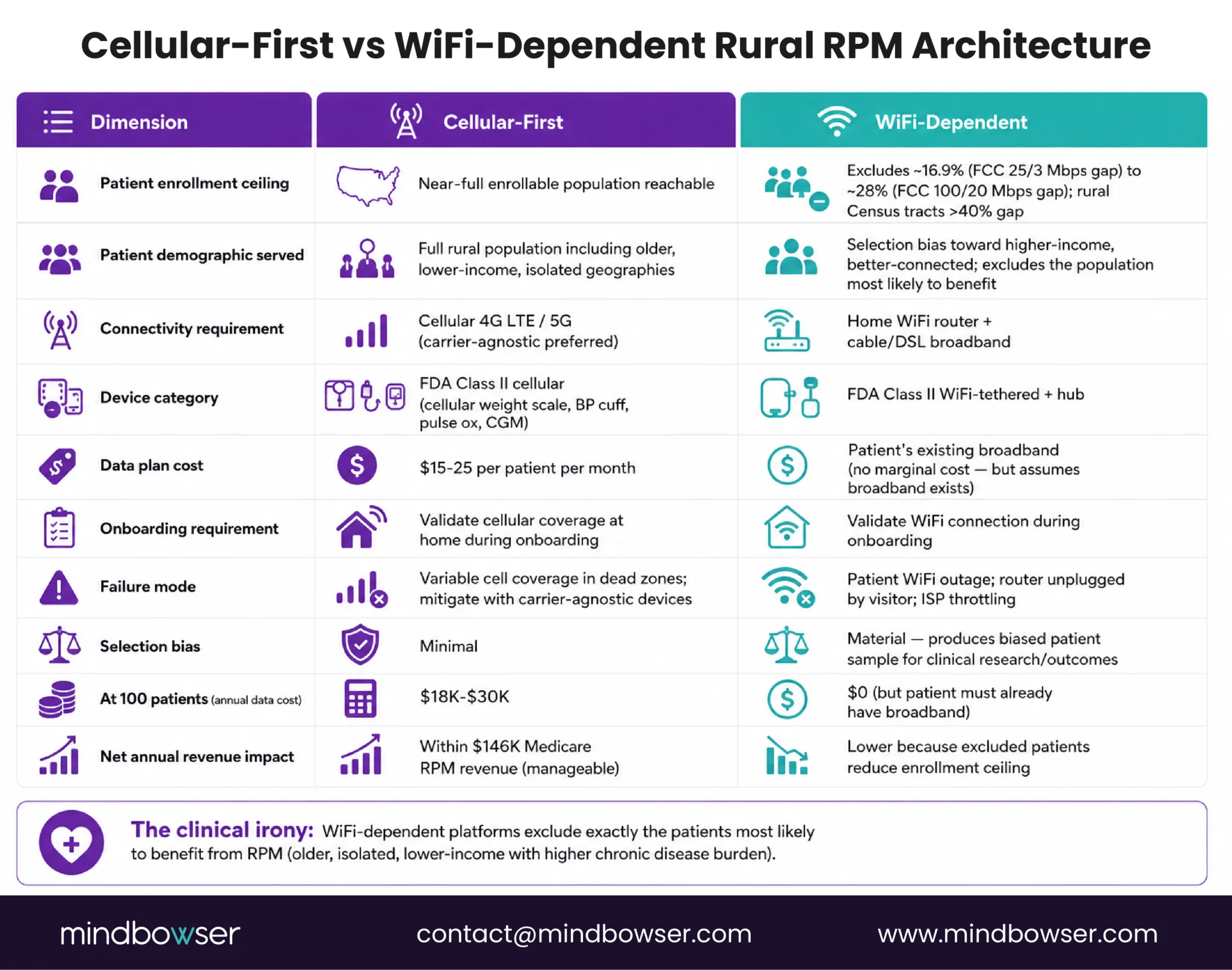
The FCC data: The FCC’s 2024 Section 706 Broadband Deployment Report tracks rural broadband access through a combination of provider reporting and direct measurement. The data shows approximately 16.9 percent of rural Americans lack fixed broadband at the older 25/3 Mbps threshold, and roughly 28 percent lack access at the current 100/20 Mbps standard that the FCC adopted in March 2024. In specific rural Census tracts, the gap at modern benchmarks exceeds 40 percent. The Rural Digital Opportunity Fund and state-level broadband expansion programs are closing the gap slowly, but the patient populations rural hospitals serve today include broadband-excluded households, and the constraint is getting more severe as the benchmark moves to 100/20.
What this means for RPM architecture:
If the RPM platform requires home WiFi for device connectivity, the program excludes roughly one in four enrollable patients at launch. The excluded patients tend to be older, lower-income, and in more isolated geographies — which correlates with higher chronic disease burden and therefore higher clinical need for RPM. The platform architectural choice produces a selection bias that harms exactly the patients RPM is designed to serve.
Cellular-first solves this:
Cellular-enabled devices transmit data over 4G LTE or 5G networks without requiring home WiFi. The devices are FDA Class II cleared with the same clinical accuracy standards as WiFi-enabled devices. Cellular data plans run $15-25 per patient per month depending on volume and carrier. At 100 enrolled patients, cellular data costs total $18K-$30K annually — material but manageable within the $120K annual Medicare RPM revenue at that patient volume.
Device manufacturer patterns:
Several medical device manufacturers produce cellular-first device lines. Specific manufacturer selection matters less than the underlying architectural pattern: the RPM platform must operate on a device-agnostic ingestion layer that supports any FDA-cleared cellular device, not a proprietary hub requiring home WiFi connectivity.
Reliability considerations:
Not all rural areas have uniform cellular coverage. Signal strength varies by geography, cell tower density, and terrain. Rural RPM programs must validate cellular coverage in the patient’s home during onboarding, not during a clinical event. Carrier-agnostic device selection (supports multiple carriers) provides fallback options in areas with variable coverage.
Which Clinical Use Cases Produce Measurable Revenue at a Rural Hospital
Rural RPM works clinically and financially for five use cases with measurable reimbursement capture at CAH scale.
Use Case 1: Congestive Heart Failure (CHF) monitoring.
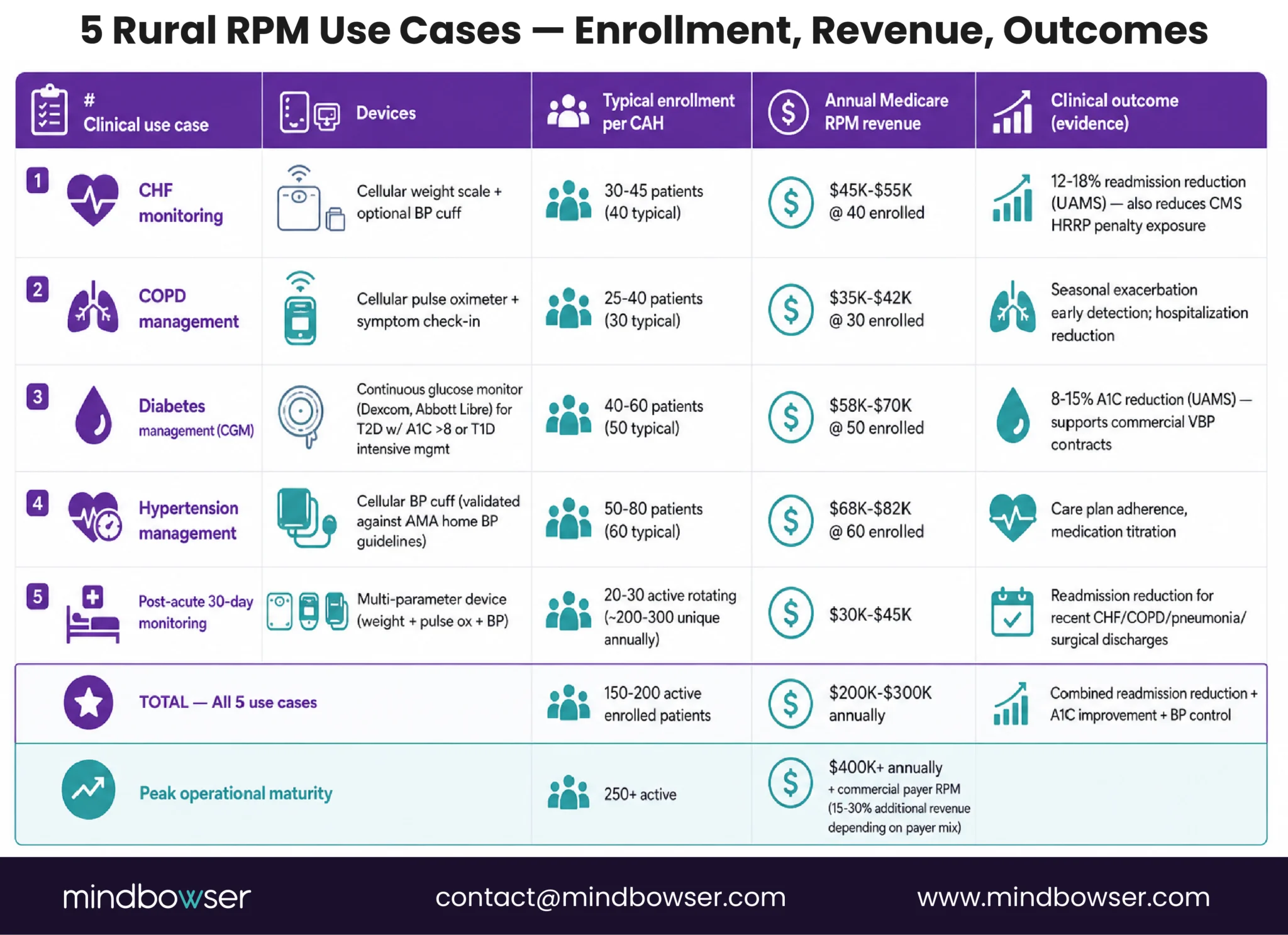
Daily weight measurement plus symptom check-in for patients with Class II-III CHF. The intervention targets readmission reduction, which matters for both clinical outcomes and CMS Hospital Readmissions Reduction Program (HRRP) penalty exposure. Typical enrollment: 30-45 CHF patients per rural hospital service area. Annual Medicare RPM revenue at 40 enrolled: $45K-$55K.
Use Case 2: COPD management.
Pulse oximetry plus symptom tracking for moderate-to-severe COPD. Seasonal exacerbation monitoring is the primary clinical value. Typical enrollment: 25-40 COPD patients. Annual Medicare RPM revenue at 30 enrolled: $35K-$42K.
Use Case 3: Diabetes management.
Continuous glucose monitoring (CGM) integration for type 2 diabetics with A1C above 8 percent or type 1 diabetics requiring intensive management. A1C improvement is the measurable outcome that supports commercial value-based payment contracts in addition to Medicare RPM billing. Typical enrollment: 40-60 diabetic patients. Annual Medicare RPM revenue at 50 enrolled: $58K-$70K.
Use Case 4: Hypertension management.
Home blood pressure monitoring for uncontrolled hypertension patients. Care plan adherence and medication titration are the clinical outcomes. Typical enrollment: 50-80 hypertensive patients. Annual Medicare RPM revenue at 60 enrolled: $68K-$82K.
Use Case 5: Post-acute monitoring (30-day post-discharge).
Short-duration RPM for patients discharged after hospitalization for specific conditions (CHF, COPD, pneumonia, surgical procedures). 30-day monitoring window targets readmission reduction. Typical enrollment: rotating 20-30 patients at any time, ~200-300 unique patients annually. Annual Medicare RPM revenue: $30K-$45K.
Combined revenue at full deployment:
A rural hospital running all five use cases at typical enrollment volumes generates $200K-$300K in annual Medicare RPM revenue from roughly 150-200 active enrolled patients. At peak operational maturity, some rural RPM programs exceed $400K annual revenue. These are Medicare-only numbers; commercial payer RPM reimbursement adds 15-30 percent depending on payer mix.
Clinical outcome evidence:
UAMS research on rural RPM deployments documents measurable clinical outcomes: 12-18 percent readmission reduction for CHF patients, 8-15 percent A1C reduction for diabetics, comparable or better medication adherence than in-clinic care. The Bipartisan Policy Center’s Maximizing RPM Value explainer documents similar outcomes at scale.
Medicare RPM Billing: CPT 99453-99458 at a Rural Hospital
Medicare RPM billing operates through four CPT codes, each covering a specific component of the RPM service. All four apply to Critical Access Hospitals and PPS rural hospitals.
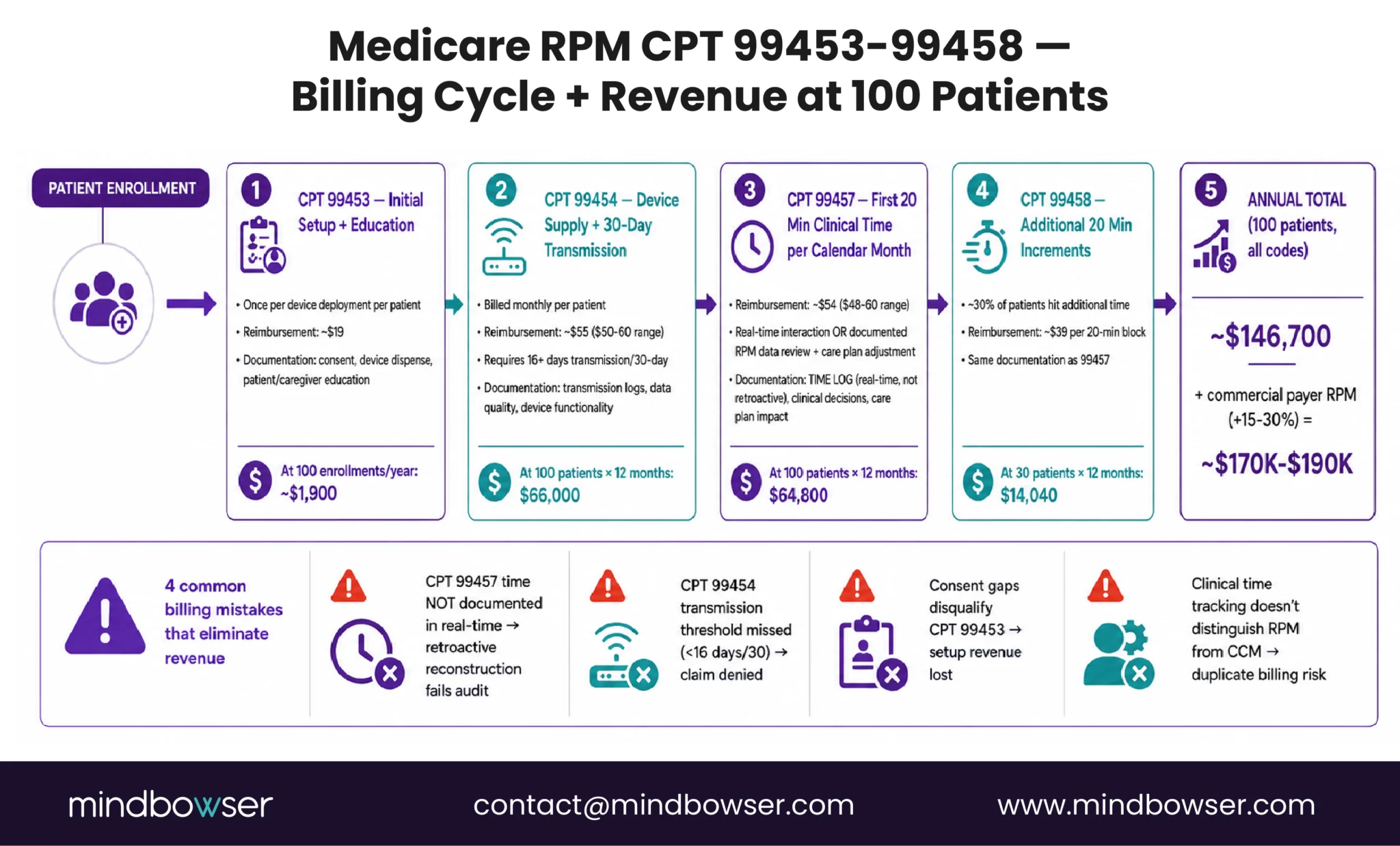
- CPT 99453 — Initial setup and patient education. Billed once per device deployment per patient episode. Reimbursement: approximately $19. Documentation requirements: patient consent, device dispensation record, patient/caregiver education delivery.
- CPT 99454 — Device supply with daily data transmission over 30-day period. Billed monthly per patient. Reimbursement: approximately $50-60. Requires at least 16 days of data transmission during the 30-day period. Documentation: transmission logs, data quality check, device functionality confirmation.
- CPT 99457 — First 20 minutes of clinical staff time managing the patient per calendar month. Reimbursement: approximately $48-60. Requires real-time interaction with patient or documentation of RPM data review and care plan adjustment. Documentation: time log, clinical decisions made, care plan impact.
- CPT 99458 — Each additional 20 minutes of clinical staff time per calendar month, billed in 20-minute increments. Reimbursement: approximately $38-40 per increment. Same documentation as 99457 with time log showing additional engagement.
Revenue calculation at 100 enrolled patients:
- 99453 (device setup, amortized): ~$19 × 100 initial setups annually = ~$1,900
- 99454 (monthly device transmission): $55 average × 100 × 12 = $66,000 annually
- 99457 (first 20 min clinical time): $54 average × 100 × 12 = $64,800 annually
- 99458 (additional time for ~30% of patients): $39 × 30 × 12 = $14,040 annually
Combined annual Medicare RPM revenue at 100 patients: approximately $146,700.
CAH-specific billing considerations:
Medicare RPM is fee-for-service outpatient billing, not cost-report-based. Revenue flows immediately as services are rendered and billed, rather than waiting for the annual Medicare Cost Report cycle. This is financially meaningful for CAH cash flow. The CPT 99457 and 99458 clinical time billing works regardless of whether the clinical staff is physician, APP, or care coordinator RN under supervision.
Common billing mistakes that eliminate revenue:
- Failure to document CPT 99457 clinical time in real-time (retroactive reconstruction fails audit)
- Missing device transmission threshold for CPT 99454 (fewer than 16 days of data in the period)
- Consent documentation gaps that disqualify the patient from CPT 99453 billing
- Clinical time tracking that does not distinguish RPM time from other chronic care management time (risk of duplicate billing)
For the deeper financial picture including how Medicare RPM revenue integrates with CAH cost-based reimbursement, see our Critical Access Hospital Reimbursement and Technology ROI guide.
The 90-Day Rural RPM Launch Sequence
The 90-day launch is achievable when device selection, clinical workflow, and EHR integration happen in parallel streams rather than sequential dependencies.
| Phase | Weeks | Deliverables | Key Risk |
|---|---|---|---|
| Foundation | 1-2 | Device vendor selection, care coordinator hiring or assignment, clinical protocols drafted, billing workflow designed | Care coordinator hiring delay (rural workforce constraint); plan for internal reassignment as backup |
| Build | 3-5 | Platform deployment, EHR integration (FHIR R4), clinical workflow implementation, initial device inventory received | EHR vendor API documentation gaps; rural EHRs (older MEDITECH, Athena) sometimes require middleware |
| Pilot | 6-8 | 10-15 initial patients enrolled, workflow calibration, first CPT 99457 billing cycle completed, onboarding friction identified | Patient onboarding dropout in first 14 days; guided onboarding mitigates |
| Scale | 9-10 | Expansion to 30-50 active patients, care coordinator workflow stabilized, staff training expanded | Alert fatigue surfaces at this scale; AI triage calibration becomes critical |
| Launch | 11-13 | Operational launch at 75-100 active patients, ongoing optimization cycles, first quarterly clinical outcome review | Billing documentation gaps surface in first claim submission cycle; dedicated billing attention in weeks 11-16 |
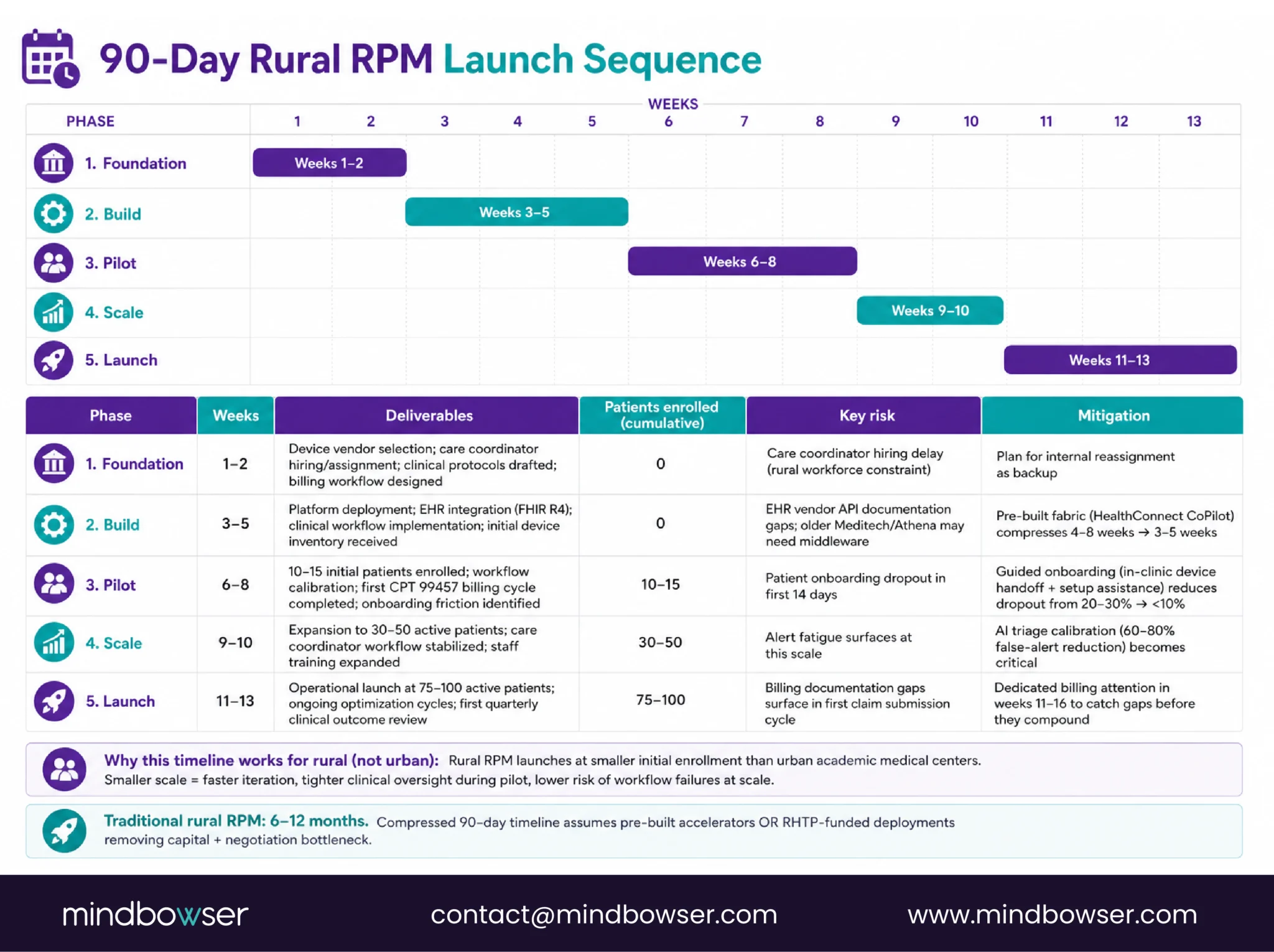
Why this timeline works for rural:
Rural RPM launches at smaller initial enrollment than urban academic medical center deployments. The smaller scale enables faster iteration, tighter clinical oversight during pilot, and lower risk of workflow failures at scale. Commercial RPM platforms and RHTP-funded deployments both support this compressed timeline.
Traditional rural RPM launches:
Most rural hospitals historically took 6-12 months to launch RPM, driven by sequential capital approval, vendor negotiation, and integration timelines. The compressed 90-day timeline assumes either pre-built platform accelerators or RHTP-funded platforms that remove the capital and negotiation bottleneck.
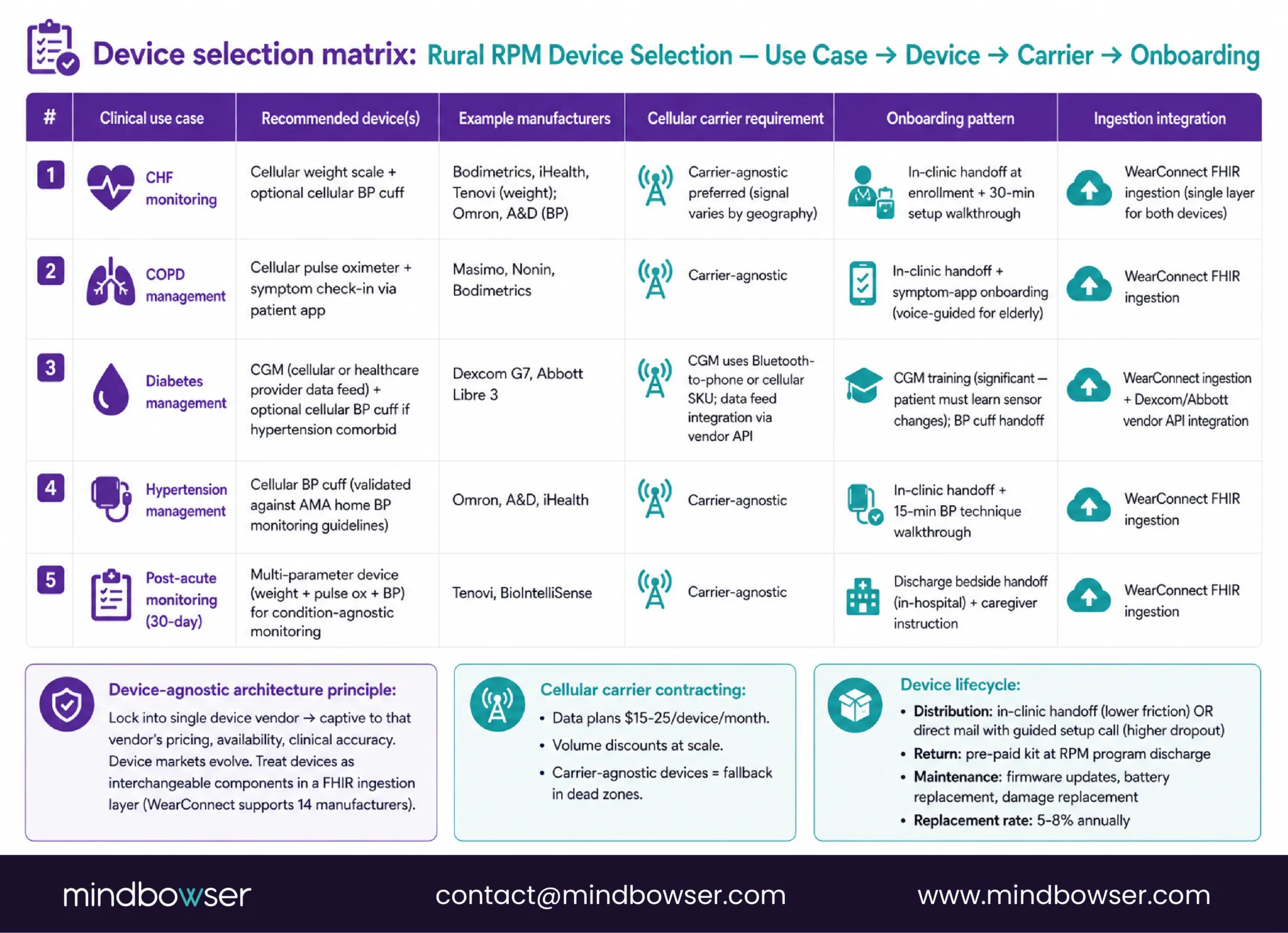
Step 1: Device Selection and Cellular Infrastructure
Device selection is where rural RPM architecture decisions either enable or constrain the program for years after launch.
The device-agnostic architecture principle:
Lock into a single device vendor and the program is captive to that vendor’s pricing, availability, and clinical accuracy. Device markets evolve. New sensors, better battery life, lower costs, different clinical indications all emerge over multi-year horizons. The RPM platform must treat devices as interchangeable components within a FHIR-compatible ingestion layer.
WearConnect supports 14 device manufacturers through a single ingestion layer. The abstraction means a rural hospital can start with one device manufacturer for CHF monitoring, add a different manufacturer for CGM diabetes monitoring, and change BP cuff vendors later, all without platform rework.
Device selection matrix by clinical use case:
- CHF: Cellular weight scale (Bodimetrics, iHealth, Tenovi) plus optional BP cuff
- COPD: Cellular pulse oximeter plus symptom check-in via patient app
- Diabetes: CGM (Dexcom, Abbott Libre) integrated via healthcare provider data feed or cellular BP cuff with medication adherence tracking
- Hypertension: Cellular BP cuff (validated against AMA home BP monitoring guidelines)
- Post-acute: Multi-parameter device (weight + pulse ox + BP) for condition-agnostic monitoring
Cellular carrier contracting:
Data plans run $15-25 per device per month. Larger rural hospitals or hospital networks negotiate volume discounts. Carrier-agnostic devices support fallback coverage in areas with variable signal strength.
Device lifecycle management:
Distribution: in-clinic handoff at enrollment or direct mail to patient with guided setup call. Return: pre-paid return kit at discharge from RPM program. Maintenance: device firmware updates, battery replacement, replacement for damaged devices. Typical device replacement rate: 5-8 percent annually.
PakarPBN
A Private Blog Network (PBN) is a collection of websites that are controlled by a single individual or organization and used primarily to build backlinks to a “money site” in order to influence its ranking in search engines such as Google. The core idea behind a PBN is based on the importance of backlinks in Google’s ranking algorithm. Since Google views backlinks as signals of authority and trust, some website owners attempt to artificially create these signals through a controlled network of sites.
In a typical PBN setup, the owner acquires expired or aged domains that already have existing authority, backlinks, and history. These domains are rebuilt with new content and hosted separately, often using different IP addresses, hosting providers, themes, and ownership details to make them appear unrelated. Within the content published on these sites, links are strategically placed that point to the main website the owner wants to rank higher. By doing this, the owner attempts to pass link equity (also known as “link juice”) from the PBN sites to the target website.
The purpose of a PBN is to give the impression that the target website is naturally earning links from multiple independent sources. If done effectively, this can temporarily improve keyword rankings, increase organic visibility, and drive more traffic from search results.
Comments are closed, but trackbacks and pingbacks are open.