Is your clinical decision support software actually improving decisions or just adding more alerts?
Healthcare leaders are under pressure to deliver better outcomes while controlling costs, yet many CDS investments fail to make a meaningful impact.
The gap is not technology; it is how well decision support fits into real clinical workflows. When guidance slows clinicians down or lacks trust, adoption drops fast.
This blog breaks down how to evaluate clinical decision support software that drives measurable impact across quality, efficiency, and value-based performance.
I. Why Clinical Decision Support Software Has Become a Strategic Buy
A. The market reality facing provider organizations and digital health leaders
Healthcare leaders are no longer buying software. They are buying outcomes.
Quality scores. Readmission penalties. Clinician burnout. Throughput bottlenecks. Every one of these now ties directly to financial performance. CMS estimates that nearly 1 in 5 Medicare patients are readmitted within 30 days, driving billions in avoidable costs. That is not just a clinical issue. It is a margin issue.
At the same time, the stack has changed.
What used to be isolated tools is now expected to operate inside connected workflows. EHRs, care management platforms, and analytics layers must work together. Decision support is no longer a pop-up. It is part of the care delivery engine.
So what happens when decisions are delayed, inconsistent, or missed?
You see it immediately. Missed care gaps. Medication errors. Delayed interventions. Lower quality scores—higher utilization.
This is why clinical decision support software has moved from “nice to have” to strategic infrastructure.
Value-based care accelerates this shift. When reimbursement ties to outcomes, every clinical decision carries financial weight. Better decisions mean better contracts, lower total cost of care, and stronger margins.
Digital health companies feel the same pressure, just in different ways.
They are not just improving care. They are building products where decision support becomes a differentiator—faster triage. Smarter care plans—more personalized engagement.
Three forces. One reality:
- Clinical quality
- Operational efficiency
- Financial performance
All converge at the point of decision.
If your decisions are not improving, your outcomes will not improve. And neither will your margins.
B. What buyers actually mean when they search for clinical decision support software
Not all “decision support” is created equal. And buyers often know this instinctively.
When someone searches for clinical decision support software, they are not looking for another alert engine. They are looking for guidance that fits into care delivery without friction.
But the terminology gets messy fast.
Is this a platform? A feature? A module inside the EHR?
Let’s break it down the way buyers actually think about it.
First, there is a clear difference between a true CDS platform and a narrow alerting tool.
- Alerting tools fire rules.
- CDS platforms orchestrate decisions across workflows.
That distinction matters. A pop-up that flags a drug interaction is useful. But a system that integrates medication safety, patient history, lab trends, and care pathways into a single guided action is where real value lies.
Second, the term clinical decision support system software usually signals something broader.
It sits across:
- EHR workflows
- Analytics engines
- Care management platforms
It is not replacing these systems. It is connecting their intelligence .
Third, the phrase decision support software is often too generic for healthcare buyers.
It could mean anything from BI dashboards to financial planning tools. That ambiguity creates risk during evaluation.
And that risk shows up later as poor fit and low adoption.
The most sophisticated buyers narrow their definition early. They ask:
- Does this system influence decisions at the point of care?
- Does it work inside clinician workflows, not outside them?
- Does it drive action, not just insight?
Because insight alone does not change outcomes. Action does.
When buyers say “clinical decision support software,” they mean a system that fits inside real workflows and changes real decisions, not just one that generates alerts.
C. The core promise and the common disappointment
Every CDS purchase starts with the same promise: better decisions, faster.
Safer prescribing. Earlier diagnosis. Cleaner care pathways. Fewer missed interventions. On paper, clinical decision support software should elevate every clinical moment.
And in controlled environments, it often does.
But reality inside hospitals and digital health platforms tells a different story.
Why do so many implementations stall after go-live?
Because the promise breaks down at the point of use.
Clinicians do not reject decision support because they dislike guidance. They reject it when:
- Alerts interrupt without context
- Recommendations lack a clear rationale
- Workflows become slower, not faster
- Signal gets buried in noise
This is where alert fatigue becomes more than a usability issue. It becomes a safety risk. Studies show that clinicians override up to 90% of alerts in some systems, suggesting that even high-value interventions are ignored.
Now, the system designed to improve decisions is no longer trusted.
That is the tipping point.
Once trust is lost, can adoption recover?
Rarely without redesign.
The gap is not technical. It is operational.
The best-performing organizations treat CDS as a workflow design problem, not just a software purchase. They focus on:
- When guidance appears
- How it is explained
- Who receives it
- What action does it drives
Because clinicians do not need more information, they need the right guidance, at the right moment, with minimal friction.
The promise of CDS is real, but only when it fits naturally into clinical workflows and earns trust over time.
II. What Clinical Decision Support Software Actually Includes
A. A practical definition for executive and clinical buyers
At its core, clinical decision support software is simple to define and hard to execute.
It delivers patient-specific guidance at the exact moment a decision is made. Not before. Not after. Right when action is required.
That guidance can come from:
- Evidence-based rules
- Clinical guidelines
- Predictive models
- Care pathways
But none of that matters if it is not usable.
What does “usable” actually mean in a clinical setting?
It means the system translates complex logic into clear, actionable direction without forcing clinicians to stop, search, or interpret.
For example:
- A medication alert that suggests a safer alternative based on renal function
- A documentation prompt that closes a care gap during a visit
- A pathway nudge that aligns treatment with current guidelines
Each of these is small. Together, they reshape outcomes.
The delivery mechanisms vary, but they all serve the same purpose:
- Alerts during ordering
- Embedded order sets
- Dashboard insights
- Documentation prompts
- Care pathway nudges
The key is not the format. It is the timing and relevance.
Because if guidance arrives too early, it is ignored. Too late, it is useless.
Leading organizations design CDS around decision moments, not features. They map where clinicians hesitate, where errors occur, and where variation creeps in. Then they insert guidance precisely there.
That is the difference between information and intervention.
Clinical decision support software is not about delivering more data. It is about delivering the right action at the exact moment it matters.
B. The major types of clinical decision support system software
Not all CDS systems solve the same problem. And that is where many buying decisions go wrong.
Executives often evaluate platforms as if they are interchangeable. They are not. Each type of clinical decision support system software targets a different moment in care and a different value driver.
So what are you actually buying?
Let’s break it down into the major operational categories.
1. Medication safety and drug interaction support
This is the most widely adopted form of CDS. It focuses on:
- Drug-drug interactions
- Allergy checks
- Dose adjustments based on labs or conditions
It directly impacts patient safety and reduces adverse drug events. The CDC estimates that adverse drug events lead to over 1 million emergency visits annually, making this category foundational.
But here is the catch. Poor tuning leads to alert fatigue fast.
2. Diagnostic support and differential guidance
These tools assist clinicians in narrowing diagnoses based on symptoms, history, and test results.
They are especially valuable in:
- Complex cases
- Rare conditions
- Early-stage detection
When done well, they reduce diagnostic errors. When done poorly, they get ignored. Trust is everything here.
3. Order set optimization and evidence-based pathway support
This is where CDS begins to drive standardization.
Instead of relying on memory, clinicians follow:
- Pre-built order sets
- Evidence-based care pathways
This improves consistency and reduces variation across providers and sites. It also directly impacts the length of stay and throughput.
4. Preventive care and risk-gap closure support
These systems identify what is missing in a patient’s care.
- Screenings
- Vaccinations
- Chronic condition monitoring
They are critical for value-based care performance, where closing care gaps improves both outcomes and reimbursement.
5. Population health and value-based care support
This is where CDS extends beyond individual encounters.
It supports:
- Risk stratification
- Readmission reduction
- Care coordination
Instead of reacting to events, organizations can act earlier.
That shift from reactive to proactive care is where real financial impact emerges.
Three categories. Three different value levers:
- Safety
- Standardization
- Financial performance
The best CDS strategy is not choosing one type. It is aligning the right type of decision support to the outcomes your organization is trying to improve.
C. Where the software should live in the workflow
Placement decides adoption. Not features.
You can have the most advanced clinical decision support software in the market, but if it sits outside the clinician’s workflow, it will fail. Quietly. Consistently.
So where should CDS actually live?
The answer is simple in theory and difficult in execution: inside the moments where decisions happen.
1. Within the EHR
This is non-negotiable.
Decision support must operate directly within the EHR because that is where clinicians:
- Review patient data
- Place orders
- Document care
If CDS requires switching screens or logging into another system, adoption drops immediately.
2. Inside clinician documentation and ordering screens
This is where precision matters.
Guidance should appear:
- During order entry
- While documenting diagnoses
- At the point of prescribing
Not before. Not after.
If a recommendation appears after the decision is already made, what value does it add?
Timing drives impact.
3. Across care management and utilization review workflows
CDS is not just for physicians.
Nurses, care managers, and utilization teams rely on structured guidance for:
- Discharge planning
- Care coordination
- Authorization decisions
Embedding CDS here improves throughput and reduces unnecessary utilization.
4. In patient outreach and longitudinal care programs
In value-based models, decisions extend beyond visits.
CDS should support:
- Care gap outreach
- Chronic disease monitoring
- Risk-based interventions
This is where organizations shift from episodic care to continuous care.
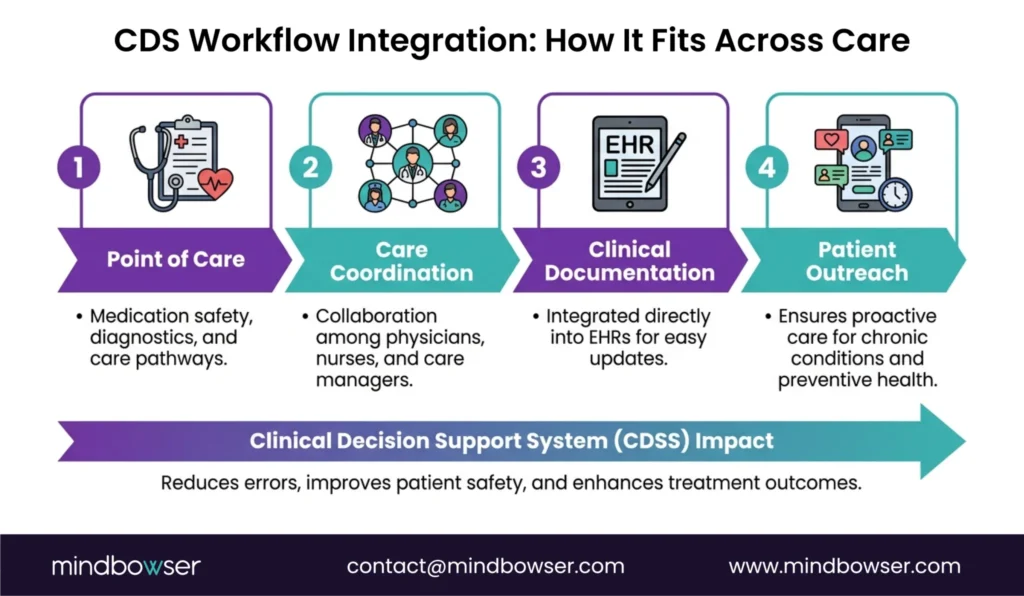
Three layers. One principle:
- Point of care
- Point of coordination
- Point of outreach
Clinical decision support software delivers value only when it is embedded directly into the workflows where decisions are made, not where reports are reviewed.
III. Why the Buying Decision Is Harder Than It Looks
A. Many tools look similar in demos
Most CDS tools win in demos. Few win in production.
On the surface, vendors show similar capabilities:
- Alerts firing at the right time
- Clean interfaces
- Evidence-backed recommendations
It looks convincing. It feels complete.
But what are you actually seeing?
A controlled environment. Clean data. Ideal workflows. No interruptions.
Real clinical environments are the opposite.
- Incomplete data
- Time pressure
- Multitasking clinicians
- Competing priorities
This is where the gap appears.
Alerting is easy to demonstrate. Sustained adoption is not.
A McKinsey analysis finds that up to 70% of digital health implementations fail to scale beyond pilot phases . CDS follows the same pattern when workflow design is weak.
The difference between tools that succeed and tools that fade into the background comes down to three factors:
- Evidence quality
- Workflow precision
- Operational fit
Does the system guide decisions without adding cognitive load?
That question rarely gets answered in a demo.
Leading buyers push beyond surface validation. They simulate real workflows. They test edge cases. They involve frontline clinicians early.
Because the goal is not to see if the tool works.
It is to see if it still works under pressure.
If your evaluation stops at the demo, you are not evaluating adoption. You are evaluating a presentation.
B. The biggest failure points buyers underestimate
Most CDS failures are predictable. Buyers just don’t catch them early enough.
On paper, the system checks every box. In reality, adoption drops, clinicians override alerts, and ROI never materializes.
Where does it actually break?
1. Alert fatigue
This is the most visible and most dangerous failure.
When clinicians are constantly interrupted, they stop engaging. Studies show override rates can exceed 90% in poorly tuned systems.
At that point, even high-risk alerts get ignored.
What starts as safety support becomes background noise.
2. Weak interoperability
CDS is only as good as the data feeding it.
If integration with:
- EHR systems
- FHIR and HL7 interfaces
- Payer and claims data
- Device and remote monitoring inputs
is incomplete or delayed, recommendations become unreliable.
And if clinicians do not trust the data, will they trust the guidance?
They won’t.
3. Poor local customization
Clinical workflows are not generic.
Service lines differ. Specialties vary. Organizational protocols evolve.
A one-size-fits-all CDS system creates friction instead of alignment.
High-performing organizations invest in local configuration and governance from day one.
4. Limited governance after go-live
Many buyers treat implementation as the finish line. It is not.
Without:
- Ongoing rule tuning
- Clinical oversight
- Performance monitoring
the system degrades over time.
What worked at launch becomes outdated within months.
5. Lack of explainability and trust
If a system cannot explain why a recommendation appears, clinicians hesitate.
Black-box logic creates doubt. Doubt kills adoption.
Especially in high-risk decisions, transparency is non-negotiable.
Three recurring failure patterns:
- Too many alerts
- Not enough trust
- No ongoing ownership
CDS does not fail because of missing features. It fails when data, workflow, and trust are not aligned from the start.
C. Why hospitals and digital health companies evaluate this differently
The same software. Two completely different buying lenses.
At first glance, both provider organizations and digital health companies evaluate clinical decision support software for similar reasons: better outcomes, faster decisions, improved efficiency.
But once you look closer, the priorities diverge quickly.
What does success actually look like for each?
1. Provider organizations: safety, throughput, and quality metrics
Hospitals and provider groups operate under constant clinical and financial pressure.
Their evaluation focuses on:
- Patient safety improvements
- Reduction in errors and adverse events
- Throughput gains and length of stay reduction
- Quality scores tied to reimbursement
For them, CDS must prove one thing clearly:
Does this improve care without slowing clinicians down?
If it adds friction, it fails.
2. Digital health companies: scale, speed, and product differentiation
Digital health companies view CDS as a product capability, not just infrastructure.
Their priorities shift toward:
- Fast integration into existing platforms
- Configurability across clients and use cases
- Ability to differentiate their offering in the market
Here, CDS becomes part of the user experience. It powers triage, care plans, engagement, and personalization.
In this context, can your product scale without intelligent decision support?
Not for long.
3. The shared requirement: measurable business value
Despite different lenses, both groups converge on one expectation:
Show measurable impact.
That means:
- Improved clinical outcomes
- Reduced unnecessary utilization
- Better value-based performance
- Clear operational efficiency gains
No matter the organization type, CDS must move beyond promise into proof.
Three perspectives. One common demand:
- Clinical trust
- Operational fit
- Financial return
Whether you are a provider or a digital health company, the right CDS solution is the one that aligns with your operating model and delivers measurable value where it matters most.
PakarPBN
A Private Blog Network (PBN) is a collection of websites that are controlled by a single individual or organization and used primarily to build backlinks to a “money site” in order to influence its ranking in search engines such as Google. The core idea behind a PBN is based on the importance of backlinks in Google’s ranking algorithm. Since Google views backlinks as signals of authority and trust, some website owners attempt to artificially create these signals through a controlled network of sites.
In a typical PBN setup, the owner acquires expired or aged domains that already have existing authority, backlinks, and history. These domains are rebuilt with new content and hosted separately, often using different IP addresses, hosting providers, themes, and ownership details to make them appear unrelated. Within the content published on these sites, links are strategically placed that point to the main website the owner wants to rank higher. By doing this, the owner attempts to pass link equity (also known as “link juice”) from the PBN sites to the target website.
The purpose of a PBN is to give the impression that the target website is naturally earning links from multiple independent sources. If done effectively, this can temporarily improve keyword rankings, increase organic visibility, and drive more traffic from search results.
Comments are closed, but trackbacks and pingbacks are open.